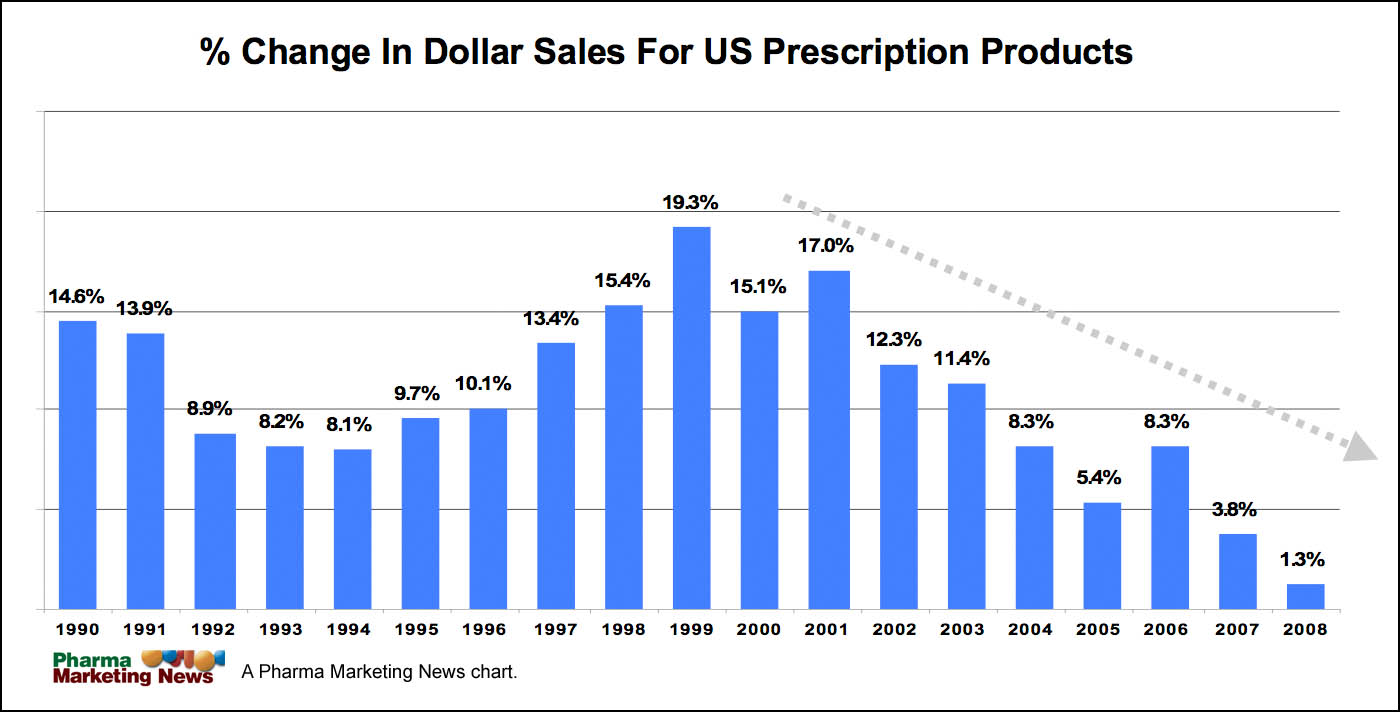
“We ration care in the US today using one of the most capricious and inequitable means possible — ability to pay,” says Kim Slocum, former Director, Strategic Planning & Business Development at AstraZeneca, in an article to be published in the March 2009 issue of Pharma Marketing News. “As cost shifting to consumers has accelerated over the past decade, we’ve seen the effects of this as year-on-year sales growth for prescription products has dropped on more or less a straight line since 2000.”
 |
| Click on image for larger view. |
To support his thesis, Slocum sent me the chart above, which shows the percent change in dollar sales for US prescription products from 1990 through 2008. The original source of this data is the IMS National Sales Perspective, January 2006, 2007, 2008, 2009.
“There’s plenty of evidence to show that the average consumer is a very inferior decision-maker when it comes to health care,” says Slocum. “Consumers tend to cut back on all sorts of care, both necessary and unnecessary, in equal proportions.”
Unless something changes, Slocum envisions dire consequences for the drug industry:
“Extend the trend out just a bit further and you’re faced with a world in which sixty or seventy million people are completely uninsured with many of the remainder living with very skimpy coverage. Generic utilization rates in this situation probably exceed 80% and perhaps 30%-40% of all prescriptions go unfilled.”
This describes a future scenario Slocum calls “Consumer Chaos.” He spoke about this and alternative scenarios in a recent Pharma Marketing Talk podcast entitled “Will Healthcare be Rationed or Rational?” In that podcast he made a case for the industry to support Comparative Effectiveness Research or CER.
CER gathers real-world evidence on what medical therapies and technologies work best and is often cited as a fix for the nation’s rising health costs. “[CER] is much discussed these days in the face of the $1 billion-plus appropriation contained in the American Recovery and Reinvestment Act (ARRA) to set up such a function here in the US,” said Slocum.
The U.S. Department of Health and Human Services (HHS) yesterday announced (here) the members of the Federal Coordinating Council for Comparative Effectiveness Research. Authorized by the American Recovery and Reinvestment Act (ARRA), the new council will help coordinate research and guide investments in comparative effectiveness research funded by the Recovery Act.
“Comparative effectiveness research can improve care for all Americans and is an important element of President Obama’s health reform plan,” said HHS Spokeswoman Jenny Backus. “President Obama is committed to openness and transparency and the Coordinating Council will host open meetings and a listening session as it begins its important work.”
It’s obvious that the pharmaceutical industry needs to get involved in the discussion since the stakes are very high. “The only real threat of CER is to have it done badly, by people whose only interest is in reducing costs,” said Slocum. PhRMA — the trade association representing the interests of US pharmaceutical companies — agrees. Yesterday, PhRMA Senior Vice President Ken Johnson issued the following statement:
“The economic stimulus law made an important footprint in the health care debate by providing significant funds for government-sponsored comparative effectiveness research (CER). PhRMA has long supported well-designed CER because when used correctly, it can serve as a tool to help improve patient outcomes and medical decision-making.
“To help ensure that CER is used to promote patient health and improve the quality of health care in the U.S., it is critical that the new Federal Coordinating Council listen carefully to input from all stakeholders throughout the process, particularly physician and patient input because, ultimately, they will be ones most impacted by the Council’s recommendations.
“As the Administration continues to implement this initiative, we expect it will be done with transparency, openness, accountability and public input in how research priorities are set and how studies are ultimately communicated and conducted.
“We look forward to working with members of Congress and the Administration as a long-term framework for comparative clinical effectiveness research is established.”
Will CER be a part of our future healthcare system? How will it be implemented? CER is just part of ONE of the possible future scenarios that Slocum envisions. For more details and to provide your input on this issue, see “Future Health Care Scenarios. Which is Best for Pharma?“











{kind=link}